


Background. The Philadelphia (Ph) chromosome (chr.) is the hallmark of chronic myeloid leukemia (CML) and typically results from the reciprocal translocation t(9;22)(q34;11.2). Complex variant translocations (CVT) involving one or more additional chr. are identified in less than 5% of newly diagnosed CML. There are conflicting reports about the prognostic impact of CVT in the achievement of optimal response to tyrosine kinase inhibitor (TKI), and very few studies addressed the role of frontline treatment with imatinib or second generation (2G)-TKI in patients with CVT.
Aims. To assess the response to imatinib or 2G-TKI in a large cohort of newly diagnosed CML with CVT, and to explore the impact of the different chr. translocations on outcome.
Methods. This observational retrospective study was conducted in 19 hematologic centers in the framework of Campus CML, a network of Italian physicians involved in the management of CML patients. All newly diagnosed CML from 2000 to 2019 were evaluated and patients with CVT were selected for the present analysis. Karyotypes were defined according to the 2016 International System for Human Cytogenetic Nomenclature. Responses to frontline treatment were retrospectively categorized according to the 2013 ELN recommendations, as they include cytogenetic milestones. Deep molecular response (DMR, i.e. MR4or better) was defined as BCR-ABLIS ratio ≤0.01% or undetectable disease with ≥10,000 ABL copies. Patients with DMR lasting ≥2 years and at least a Q-PCR test every 6 months were defined as stable DMR responders. Failure-free survival (FFS) was calculated from the start of frontline TKI treatment to progression to advanced phase, death, or switch to other treatments for resistance. For FFS calculation, patients were censored at TKI stop for treatment-free remission (TFR) or in case of switch for intolerance only. Differences between subgroups according to the partner chr. were presented for descriptive purposes.
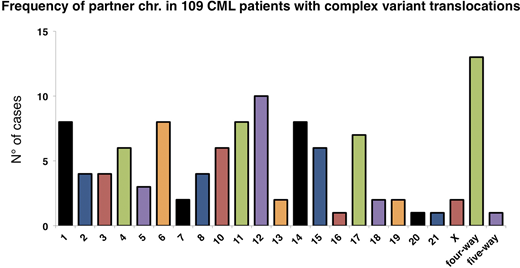
Results. CVT were identified in 109 (3.2%) patients from a whole population of 3,361 subjects with newly diagnosed CML. Ninety-five out of 109 patients (87%) exhibited three-way translocations, with chr. 1, 4, 6, 10, 11, 12, 14, 15 and 17 representing the most common additional partners (figure). Four- and five-way translocations were identified in 13 and 1 patients, respectively. Additional chr. abnormalities (ACA) in the Ph+ cells were observed in 15/109 (13.8%) patients and were more common in older individuals (p=0.018).
Overall, median age at diagnosis was 50.6 years (range 20-90). Risk distribution according to the ELTS score was 54%, 28% and 8% for L, I and H risk, respectively (10% missing). Cytogenetic result was available before the choice of frontline treatment in 45% of cases and represented a decisive factor in 28% of them (i.e. clinicians selected a 2G-TKI or high-dose imatinib, according to the available options). Frontline TKI treatment was imatinib in 80 cases (73%) and 2G-TKI (nilotinib n=22, dasatinib n=6, bosutinib n=1) in the remaining cases. The frequency of optimal response at 3, 6 and 12 months was 48%, 45% and 53%, respectively, for imatinib-treated patients, and 76%, 83% and 76%, respectively, for the 2G-TKI cohort (p<0.05 for all comparisons). Stable DMR was achieved by 39% of patients and 42% of them attempted a TFR. After a median follow-up of 91.3 months (range 1-236), 5-year FFS was 66% (95%CI: 53.4-76.4) and 84% (95%CI: 62.4-93.6) for imatinib and 2G-TKI treated patients, respectively (p=ns). The estimated 10-year OS for the entire cohort was 84.4% (95%CI: 73.6-91).
The subtype of CVT had an impact on response and long-term outcome. Patients with CVT involving chr. 1, 4, 6, 11 or 12 had a higher frequency of MMR at 12 months than patients with CVT involving chr. 10, 14, 15 or 17 (75.8% vs 30.4%, respectively, p=0.001), higher frequency of stable DMR (48.7% vs 22.2%, respectively; p=0.04) and tended to have better median FFS (p=0.07), regardless of the type of frontline TKI and of the ELTS score.
Conclusions. Due to its retrospective nature, this study does not allow to define which is the optimal therapy for CML harboring CVT at diagnosis. However, our data reinforce the usefulness of bone marrow karyotyping in CML. The observed differences between partner chr. may also depend on the breaking points, which are variable. Further dissection of CVT will help to identify which are associated to a poor response to TKIs.
D'Adda:Incyte: Other: Advisory board; Novartis: Other: Advisory board; Pfizer: Other: Advisory board. Galimberti:Novartis: Speakers Bureau; Incyte: Honoraria. Crugnola:Celgene: Honoraria; Janssen: Honoraria; BMS: Honoraria; Novartis: Honoraria. Bocchia:Incyte: Honoraria; CELGENE: Honoraria. Krampera:Janssen: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Breccia:Incyte: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Abbvie: Consultancy; Bristol-Myers Squibb/Celgene: Consultancy, Honoraria; Novartis: Consultancy, Honoraria. Saglio:Novartis: Research Funding; Ariad: Research Funding; Pfizer: Research Funding; Bristol-Myers Squibb: Research Funding; Incyte: Research Funding; Roche: Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal